Relationships of Sagittal Skeletal Discrepancy, Natural Head Position, and Craniocervical Posture in Pakistani Children
By Hafsa Abdul Ghafoor, Syed Sheeraz HussainAffiliations
doi: 10.29271/jcpsp.2024.03.313ABSTRACT
Objective: To assess the natural head position (NHP), mean sagittal skeletal discrepancy, and craniocervical posture in children presenting to tertiary care hospital.
Study Design: Observational study.
Place and Duration of the Study: Department of Orthodontics, Karachi Medical and Dental College, Karachi, Pakistan, from January to April 2022.
Methodology: A total of 121 participants, of either gender aged 11 to 15 years, were selected for this study. The mean age of the participants was 13.4 ± 1.2 years, and their average Frankfort mandibular plane angles (FH/ML) were recorded. Data collection took place following approval from the Ethics Review Board (ERB), and verbal informed consent was obtained from all participants. Cephalometric radiographs were taken in the natural head position (NHP) for all 121 participants. Based on their ANB angles, the participants were categorised into skeletal classes I, II, and III. The study assessed and compared variables such as head posture, craniocervical posture, and sagittal craniofacial morphology.
Results: The study included a sample of 121 children with a mean age of 13.4 ± 1.2 years. Among the participants, 58% were males, while 42% were females. Based on their ANB angles, participants were classified into skeletal classes I (n=44), II (n=73), and III (n=4). The correlation analysis between craniofacial posture, natural head position, and sagittal skeletal classes (I, II, and III) did not reveal any statistically significant results. Moreover, within each skeletal class, there were no significant differences observed in craniocervical posture between males and females when considering demographic variables.
Conclusion: This study indicates that there is no discernible difference in the craniocervical posture of young Pakistani children aged 11 to 15 years, regardless of gender, in relation to skeletal relationships in classes I, II, and III. These findings suggest that sagittal skeletal discrepancies may not significantly impact craniocervical posture in this particular age group.
Key Words: Craniocervical posture, Sagittal discrepancy, Natural head position.
INTRODUCTION
Cephalometric analysis often utilises reference planes, such as the sella-nasion (SN) and Frankfort (FH) horizontal planes, to assess the vertical or sagittal skeletal relationship. However, these planes can change with growth and may provide misleading information. As an alternative, the true vertical plane is used.1,2
A standardised head position, known as the natural head position (NHP), is defined as when an individual looks at a distant object at eye level with an upright head.1-3
It serves as a reliable reference due to its good reproducibility in each individual with respect to a true vertical line. Previous studies have indicated that the reproducibility of NHP remains reliable even after 5-10 minutes, 5 years, or even 15 years.4
An individual's natural head position and craniocervical posture are determined by neuromuscular balance and their body's response to environmental and physiological circumstances. Changes in head and craniocervical position have been associated with nasal obstruction, temporomandibular disorders (TMD), and bruxism due to the anatomical and mechanical connection between the cervical spine, dento-facial tissues, and head position.5
Numerous studies have investigated the relationship bet-ween sagittal skeletal discrepancy,3 NHP, and craniocervical posture.1,2,6-10 These studies have shown that nasal obstructions result in an elevation of the head relative to the cervical column and the true vertical line. Conversely, reduced nasal resistance from corticosteroid treatment, adenoidectomy, or rapid maxillary expansion leads to a decrease in craniocervical angulation and a flexion of the head.1,2,9 It has also been documented that individuals with TMD tend to exhibit an increased craniocervical angulation and a pronounced forward inclination of the upper cervical spine, while bruxers display a more anterior and downward tilt of the head.1,7,11
Based on the findings of previous studies, NHP and craniocervical posture are associated with various dento-skeletal malocclusions, orthopaedic treatments, and orthognathic surgeries. Additionally, it has been demonstrated that variations in craniocervical posture during growth are linked to changes in the pattern of facial skeleton development and that facial development in individuals with large or small craniocervical angles may be somewhat predictable.1,2,6,7
This study aimed to explore the interconnections among NHP, cranio cervical posture, and sagittal skeletal discrepancy in young Pakistani children exhibiting average vertical face patterns. It is noteworthy that, at the inception of the study, no local data on this specific topic were available, and the application of international values to the population under investigation was deemed inappropriate due to inherent genetic and anatomical differences. Consequently, the research sought to address this knowledge gap and contribute valuable insights specific to the Pakistani paediatric demographic.
The results obtained from this research are pivotal in shedding light on the influence of cranio cervical posture on craniofacial morphology. By delving into these relationships, the study contributes to the foundational knowledge required for future inquiries in this field. The findings not only serve as a baseline for further investigations but also pave the way for improved management strategies and more precise outcomes in the assessment and treatment of craniofacial issues in young Pakistani children. The aim of this study was to assess the natural head position (NHP), mean sagittal skeletal discrepancy, and craniocervical posture in children presenting to tertiary care hospital.
METHODOLOGY
This study was conducted after receiving approval from the Ethics Committee of the Karachi Medical and Dental College (KMDC). Following approval, data of 121 patients who met the inclusion criteria and reported to the Orthodontics Department at KMDC between January and April 2022 were analysed. The sample size was determined using the WHO sample size calculator, considering the statistics of the mean NSL/OPT angle in skeletal class III patients as 95.55°± 5.6°, with a margin of error of 1 at a confidence interval of 95%, which resulted in a sample size of 121. The inclusion criteria consisted of patients of both genders, aged 11-15 years, of Pakistani ethnic origin, who were nose breathers with complete dentition, average Frankfort mandibular plane angle (FH/ML), and belonged to Angle classes I, II, or III. Patients with a history of orthodontic treatment, wounds, burns, or scar tissue in the face and neck region, as well as those with craniofacial pathology such as TMD, were excluded from the study.
Verbal informed consent was obtained from the patients. Pretreatment cephalometric radiographs of the 121 subjects were collected using a standard technique. These subjects were categorised into skeletal relationships of classes I, II, and III based on ANB angles. Subjects with normal SNA and SNB values were assigned to the skeletal class I relationship (Group 1 = 44 patients), while subjects with a normal SNA value and a small SNB value were assigned to the skeletal class II relationship (Group 2 = 73 patients). Subjects with a small SNA value and a normal SNB value were assigned to the skeletal class III relationship (Group 3 = 4 patients). A single investigator manually conducted anatomic tracings and recorded dento-skeletal landmarks on a pre-designed proforma (Figure 1).
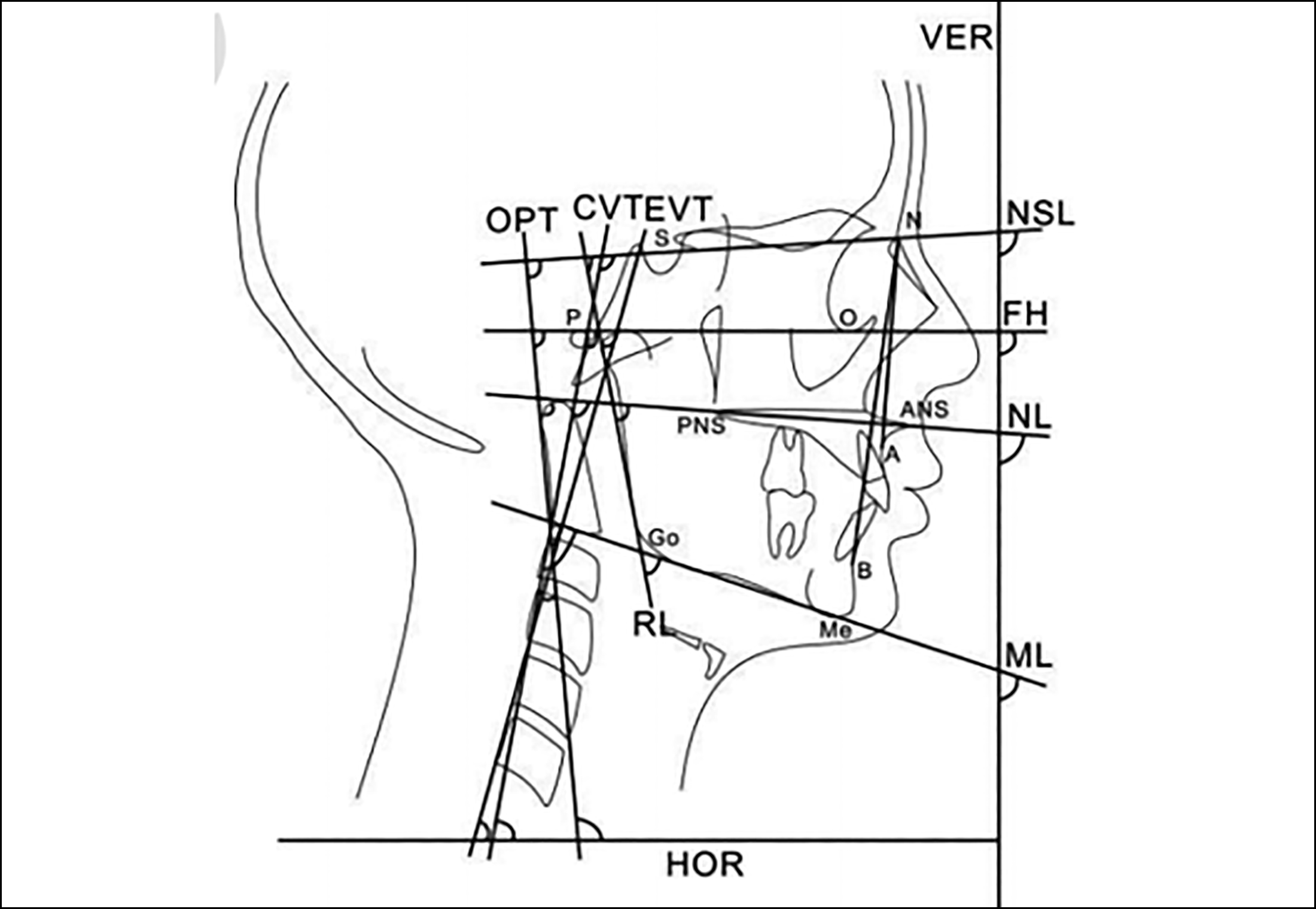 Figure 1: Cephalometric tracing illustrating all angular measurements. The definitions of the postural angles are indicated.
Figure 1: Cephalometric tracing illustrating all angular measurements. The definitions of the postural angles are indicated.
All cephalometric radiographs were manually traced by a single investigator for subsequent measurements. NSL/VER and ML/VER measurements were used to assess the natural head position. The ANB angle was used to evaluate sagittal skeletal discrepancy, while NSL/OPT, NSL/CVT, ML/OPT, and ML/CVT measurements were used to assess the craniocervical posture in the research subjects. Statistical analysis was performed using the Statistical Package for Social Sciences (SPSS), version 24.0 (SPSS Inc, Chicago, IL, USA). Categorical variables were expressed as counts and percentages, and continuous variables were expressed as mean and standard deviation (SD). The normality of the data was tested using the Shapiro-Wilk test. One-way ANOVA was applied to investigate the relationship between the variables representing the skeletal class, craniocervical posture, and natural head position. A p-value ≤0.05 was considered significant.
RESULTS
Based on the inclusion criteria, a total of 121 subjects, consisting of 84 (69.4%) females and 37 (30.6%) males, were included in this study. The mean age of the participants was 13.04 ± 1.23 years. The majority of the participants were classified as skeletal Class II (n=73), followed by skeletal Class I (n=44) and skeletal Class III (n=4).
Table I: Descriptive statistics of Sagittal skeletal pattern and variables.
|
Variables |
Sagittal Skeletal Class |
Mean (degree) |
p-values |
|
|
Craniocervial Posture |
NSL/OPT |
ClassI (n=44) |
105.23° ± 8.5° |
0.394 |
|
ClassII (n=73) |
103.20° ± 9.3° |
|||
|
ClassIII (n=4) |
107.25° ± 11.6° |
|||
|
NSL/CVT |
ClassI (n=44) |
115.61° ± 8.4° |
0.413 |
|
|
ClassII (n=73) |
113.38° ± 8.8° |
|||
|
ClassIII (n=4) |
114.50° ± 12.9° |
|||
|
ML/OPT |
ClassI (n=44) |
72.59° ± 7.9° |
0.221 |
|
|
ClassII (n=73) |
69.60° ± 9.5° |
|||
|
ClassIII (n=4) |
71.00° ± 11.1° |
|||
|
ML/CVT |
ClassI (n=44) |
82.88° ± 7.8° |
0.211 |
|
|
ClassII (n=73) |
80.08° ± 8.8° |
|||
|
ClassIII (n=4) |
82.50° ± 6.8° |
|||
|
Natural Head Position (NHP) |
NSL/VER |
ClassI (n=44) |
100.27° ± 7.4° |
0.431 |
|
ClassII (n=73) |
98.53° ± 8.9° |
|||
|
ClassIII (n=4) |
102.25° ± 9.8° |
|||
|
ML/VER |
ClassI (n=44) |
68.63° ± 8.5° |
0.165 |
|
|
ClassII (n=73) |
65.63° ± 8.1° |
|||
|
ClassIII (n=4) |
68.00° ± 11.6° |
|||
|
Sagittal Skeletal Angle |
Angle ANB |
ClassI (n=44) |
2.55° ± 1.4° |
|
|
ClassII (n=73) |
6.89° ± 1.5° |
|||
|
ClassIII (n=4) |
-1.25° ± 0.5° |
|||
|
*One-way ANOVA test is applied in the above table. |
||||
Table II: Relationship of craniocervial posture and NHP with gender.
|
Variables |
Gender |
Mean Values (degree) |
p-value |
|
|
Craniocervial Posture |
NSL/OPT |
Males |
99.97° ± 8.3° |
0.001 |
|
Females |
105.88° ± 8.8° |
|||
|
NSL/CVT |
Males |
110.16° ± 8.68° |
0.001 |
|
|
Females |
116.02° ± 8.3° |
|||
|
ML/OPT |
Males |
67.00° ± 7.3° |
0.002 |
|
|
Females |
72.38° ± 9.2° |
|||
|
ML/CVT |
Males |
78.00° ± 8.1° |
0.006 |
|
|
Females |
82.58° ± 8.3° |
|||
|
Natural Head Position (NHP) |
NSL/VER |
Males |
96.43° ± 8.1° |
0.012 |
|
Females |
100.55° ± 8.3° |
|||
|
ML/VER |
Males |
63.95° ± 6.4° |
0.012 |
|
|
Females |
68.06° ± 8.9° |
|||
|
*One-way ANOVA test is applied in the above table. |
||||
The average value of the ANB angle, which represents the sagittal facial pattern, was found to be 2.55° ± 1.4°, 6.89° ± 1.49°, and -1.25° ± 0.5° for skeletal classes I, II, and III, respectively. The mean values of the craniocervical posture determinants, namely ML/OPT, ML/CVT, NSL/OPT, and NSL/CVT, were recorded as 70.73° ± 8.9°, 81.18° ± 8.45°, 104.07° ± 9.05°, and 115.14° ± 13.41°, respectively.
The Shapiro-Wilk test, along with visual inspections of histograms and normal Q-Q plots, supported the acceptance of the alternate hypothesis that the data for dependent variables NSL/OPT, NSL/CVT, ML/OPT, ML/CVT, NSL/VER, and ML/VER were normally distributed across skeletal classes I, II, and III. One-way ANOVA was applied to examine the relationship between the variables representing skeletal class, craniocervical posture (NSL/OPT, NSL/CVT, ML/OPT, ML/CVT), and natural head position (NSL/VER, ML/VER). The resulting p-values of 0.394, 0.413, 0.221, and 0.211 were obtained via One-way ANOVA between craniocervical posture (NSL/OPT, NSL/CVT, ML/OPT, ML/CVT) and skeletal class, while p-values of 0.431 and 0.165 were obtained when the variables of natural head position (NSL/VER, ML/VER) were correlated with the skeletal class. Since all the p-values were above 0.05, the null hypothesis was accepted, indicating no relationship between skeletal class and either craniocervical posture or natural head position (Table I).
When both craniocervical posture and natural head position (NHP) were correlated with gender, statistically significant differences were observed with p-values <0.05, respectively (Table II).
DISCUSSION
The relation of neck position and forehead, along with the convexity or concavity of individual profiles in overall facial aesthetics, was evident nowadays as many studies reported the role of neck position and postero-anterior position of the forehead affecting the aesthetic profile of individuals with different jaw relations.12 Angle ANB was considered the most common modality to measure skeletal discrepancies; however, this did not account for the jaw rotation relative to reference lines, such as the Sella-Nasion line, within the skull, which affected angle ANB.13 This study also used the ANB to discriminate the three skeletal classes, i.e., Class I, II, and III, and there could have been some bias incorporated into the data due to the aforementioned jaw rotations.
Controversy exists when considering the influence of craniocervical posture and NHP on the gender variable.14 Although this study indicated that there was some statistically significant influence of gender on both the previously stated variables, the reason for the significant differences could be because of the variability in the vertical facial patterns as previously stated by Liu et al.15
Pretreatment cephalometric radiographs of patients coming under the inclusion criteria were used in this study. A debatable argument exists about the precision of this technique as it illustrates three-dimensional anatomic hard tissues in two-dimensional radiographs.1 Contrary to this, cephalo-metry was chosen for this study solely because of convenience, minimal exposure to radiation, and low cost.16
Average values of NSL/OPT in skeletal Class I, II, and III were reported to be 95.42° ± 6.38°, 98.22° ± 6.80°, and 95.55° ± 5.66°, respectively, by Liu et al., while this study showed them to be 105.22° + 8.5°, 103.20° + 9.3°, and 107.25° + 11.6° for skeletal Classes I, II, and III, respectively.1 The huge difference between the values of these studies can be because of the difference in the overall anatomical origin of the participants, i.e., Pakistani and Chinese origin.
Older studies on craniocervical posture tended to divide the participants by age.14 Contrary to this approach, this study did not do so because of the fact that the standard deviation of age was relatively small, i.e., 1.5 years, suggesting that the participants could be considered to be of the same age.
Studies about the relationships between head posture and craniofacial morphology have suggested that the craniocervical posture may influence craniofacial development.17-19 Showfety et al. suggested that maxillary and mandibular incisors and mean incisor overjet, as well as anteroposterior molar discrepancy showed no statistically significant differences between different head postures. This indicates that dental–alveolar discrepancy had no influence on head posture.20,21 In the present study, the authors investigated the relationships of craniofacial morphology, NHP, and craniocervical posture among different sagittal skeletal relationships in young Pakistani children. However, given the cross-sectional nature of this study, it is impossible to draw any firm conclusions on the aetiology or cause-and-effect relationships of the observed phenomena.
The use of a two-dimensional cephalometric imaging approach for the assessment was a drawback of the current study. The use of 3D CBCT and MRI may offer more precise information in this area as a result of technological advancements.
CONCLUSION
The findings of this study showed that there is no statistically significant variation in craniocervical position among young Pakistani children with skeletal relationships in classes I, II, and III.
ETHICAL APPROVAL:
This study was conducted after receiving approval from the Ethical Committee of the Karachi Medical and Dental College.
PATIENTS’ CONSENT:
Informed consent was obtained from all participants.
COMPETING INTEREST:
The authors declared no conflict of interest.
AUTHORS’ CONTRIBUTION:
HAG: Contributed substantially to the conception and design of the study, acquisition of data, analysis, and interpretation.
SSH: Helped and supervised the project and provided critical revision of the manuscript.
All authors approved the final version of the manuscript to be published.
REFERENCES
- Liu Y, Sun X, Chen Y, Hu M, Hou X, Liu C. Relationships of sagittal skeletal discrepancy, natural head position, and craniocervical posture in young Chinese children. Cranio 2016; 34(3):155-62. doi: 10.1179/2151090315Y.00000 00015.
- Hedayati Z, Paknahad M, Zorriasatine F. Comparison of natural head position in different anteroposterior malocclusions. J Dent (Tehran) 2013; 10(3):210-20.
- Sreenivasagan S, Sivakumar A. FSA Angle: A soft tissue approach for assessing sagittal skeletal discrepancy. Int J Clin Pediatr Dent 2021; 14(Suppl 1):54-6. doi: 10.5005/jp-journals-10005-2017.
- Peng L, Cooke MS. Fifteen-year reproducibility of natural head posture: A longitudinal study. Am J Orthod Dentofacial Orthop 1999; 116(1):82-5. doi: 10.1016/s0889-5406(99) 70306-9.
- Solow B, Kreiborg S. Soft-tissue stretching: A possible control factor in craniofacial morphogenesis. Scand J Dent Res 1977; 85(6):505-7. doi: 10.1111/j.1600-0722. 1977. tb00587.x.
- Sandoval C, Díaz A, Manríquez G. Relationship between craniocervical posture and skeletal class: A statistical multivariate approach for studying Class II and Class III malocclusions. Cranio 2021; 39(2):133-40. doi: 10.1080/08869634. 2019.1603795.
- Kamal AT, Fida M. Evaluation of cervical spine posture after functional therapy with twin-block appliances: A retrospective cohort study. Am J Orthod Dentofacial Orthop 2019; 155(5):656-61. doi: 10.1016/j.ajodo.2018.06.012.
- Bernal LV, Marin H, Herrera CP, Montoya C, Herrera YU. Craniocervical posture in children with class I, II, and III skeletal relationships. Pesqui Bras Odontopediatria Clin Integr 2017; 17(1):30-8. doi:10.4034/PBOCI.2017.171.07
- Vukicevic V, Petrovic D. Relationship between head posture and parameters of sagittal position and length of jaws. Med Pregl 2016; 69(9-10):288-93. doi: 10.2298/mpns16102 88v.
- D'Attilio M, Caputi S, Epifania E, Festa F, Tecco S. Evaluation of cervical posture of children in skeletal class I, II, and III. Cranio 2005; 23(3):219-28. doi: 10.1179/crn.2005.031.
- Paço M, Duarte JA, Pinho T. Orthodontic treatment and craniocervical posture in patients with temporomandibular disorders: An observational study. Int J Environ Res Public Health 2021; 18(6):3295. doi: 10.3390/ijerph18063295.
- Salehi P, Oshagh M, Aleyasin Z, Pakshir H. The effects of forehead and neck position on esthetics of class I, II, and III profiles. Int J Esthet Dent 2014; 9(3):412-25.
- Yassaei S, Emami A, Mirbeigi S. Cephalometric association of mandibular size/length to the surface area and dimensions of the frontal and maxillary sinuses. Eur J Dent 2018; 12(2):253-61. doi: 10.4103/ejd.ejd_345_17.
- Hellsing E, Reigo T, McWilliam J, Spangfort E. Cervical and lumbar lordosis and thoracic kyphosis in 8, 11 and 15-year-old children. Eur J Orthod 1987; 9(2):129-38. doi: 10.1093/ ejo/9.2.129.
- Liu Y, Wang S, Wang C, Liu C. Relationships of vertical facial pattern, natural head position and craniocervical posture in young Chinese children. Cranio 2018; 36(5): 311-7. doi: 10.1080/08869634.2017.1345461.
- Ansar J, Maheshwari S, Verma SK, Singh RK, Agarwal DK, Bhattacharya P. Soft tissue airway dimensions and craniocervical posture in subjects with different growth patterns. Angle Orthod 2015; 85(4):604-10. doi: 10.2319/042314- 299.1.
- Solow B, Siersbaek-Nielsen S. Growth changes in head posture related to craniofacial development. Am J Orthod 1986; 89(2):132-40. doi: 10.1016/0002-9416(86)90089-8.
- Dubojska AM, Smiech-Slomkowska G. Natural head position and growth of the facial part of the skull. Cranio 2013; 31(2): 109-17. doi: 10.1179/crn.2013.018.
- Gomes Lde C, Horta KO, Gonçalves JR, Santos-Pinto AD. Systematic review: Craniocervical posture and craniofacial morphology. Eur J Orthod 2014; 36(1):55-66. doi: 10.1093/ ejo/cjt004.
- Showfety KJ, Vig PS, Matteson S, Phillips C. Associations between the postural orientation of sella-nasion and skeletodental morphology. Angle Orthod 1987; 57(2):99- 112. doi: 10.1043/0003-3219(1987)057<0099:ABTPOO>2.0.CO;2.
- Alexa VT, Fratila AD, Szuhanek C, Jumanca D, Lalescu D, Galuscan A. Cephalometric assessment regarding craniocervical posture in orthodontic patients. Sci Rep 2022; 12(1): 21729. doi: 10.1038/s41598-022-26243-6.